There’s a particular kind of product that seems to distrust its own best feature, and once you notice it you start seeing it everywhere. The sports car with a speed limiter built into the engine. The knife that ships with a blade guard nobody asked for. Something in the design admits, quietly, that the thing it does well is also the thing that could hurt you.
Tesofensine turns out to be one of those products, except it’s a molecule instead of an object, and the stakes are a person’s heart rate rather than a fender bender. I want to spend some time with that idea, because once you see it, the whole argument for calling something “supervised” access, rather than just “access,” stops sounding like caution for its own sake and starts sounding like common sense applied to a specific, documented fact pattern.
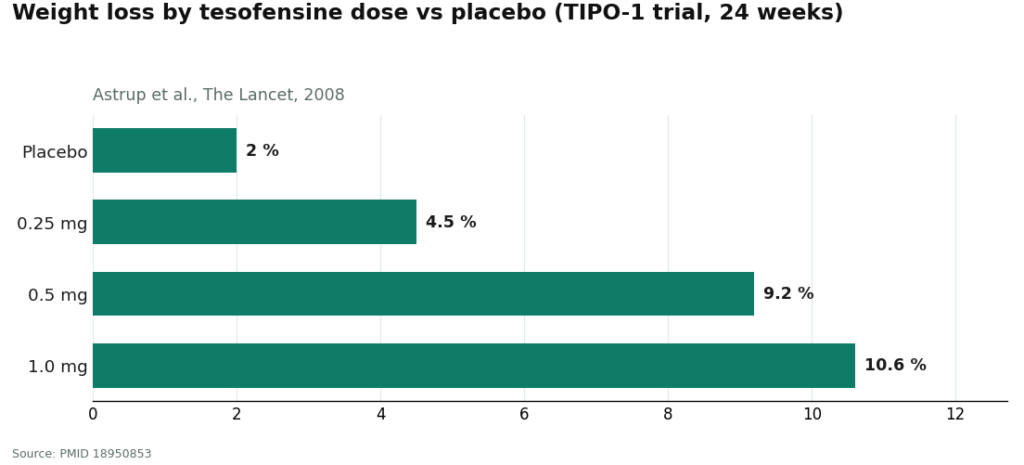
Here’s the fact pattern. In the trial that made tesofensine famous, the 2008 TIPO-1 study, the dose that produced the best weight-loss number, a 1.0 mg dose that took participants down about 10.6% versus 2.0% on placebo, was also the dose the developers walked away from, because it pushed blood pressure up more than they were willing to live with [P1]. Not a regulator killed it. Not a lawsuit killed it. The people who invented the drug looked at their own best result and decided it cost too much. That’s the first hedge.
The second hedge is stranger, and to my mind more telling. The same company that built tesofensine later built a second study, this one pairing tesofensine with a beta blocker, in an attempt to cancel out the heart-rate increase the first drug reliably produces. The study’s own language called heart rate “the most affected safety endpoint” of the compound, and the study itself was halted over safety concerns [P5]. Sit with that for a second. A company made a drug, watched it speed up the heart, and then tried to build a second drug whose job was to quiet the first one down. That is not the behavior of people who consider the side effect a footnote.
So when people ask what “supervised” is supposed to mean here, beyond a phrase stamped on a landing page, this is my answer: supervision is the thing standing in for the correction the drug’s own makers were trying, and failing, to build into a pill. A clinician watching your numbers is doing, informally and individually, roughly what that beta-blocker trial was trying to do systemically. Somebody has to argue with the drug on your behalf, because the drug, left alone, does not argue with itself convincingly enough.
Why the argument needs a referee
The mechanism explains why the stakes are cardiovascular rather than, say, digestive. Tesofensine is a triple monoamine reuptake inhibitor. It keeps serotonin, norepinephrine, and dopamine hanging around longer in the brain, which is the same broad neurochemical territory that stimulants and antidepressants work in. That’s why it suppresses appetite so effectively. It’s also, not coincidentally, why it raises heart rate.
The numbers aren’t hidden. In the TIPO-1 trial, heart rate rose by about 7.4 beats per minute at the 0.5 mg dose [P1]. A separate 2008 analysis, run in patients with Parkinson’s and Alzheimer’s who weren’t dieting at all, found the same kind of heart-rate rise, which tells you something important: this isn’t the body’s response to losing weight fast. It’s the drug itself doing it, independent of the scale [P2]. And the PET imaging work, showing dose-dependent occupancy of dopamine transporters as high as roughly 77%, gives a physical picture of just how much of the brain’s reward and arousal chemistry the drug is actually touching [P3]. The animal research points to alpha-1 adrenergic and dopamine D1 pathways as the likely drivers of the appetite effect [P4]. None of this is exotic pharmacology. It’s just pharmacology that needs a witness.
What a real intake is actually doing
If supervision is the referee, the intake appointment is where the referee learns the rules of the specific match they’re about to watch. A clinician doing this properly isn’t collecting a form. They’re establishing three things.
First, where your heart rate and blood pressure sit before any of this starts. Since the drug’s whole known cost is cardiovascular, you need a number to compare against later, and if that starting number is already high, the honest answer might be that this isn’t for you.
Second, what else you’re taking. This is the step that quietly catches the most people, because tesofensine’s effect on serotonin means it collides badly with drugs an enormous number of people are already on. Mixed with an MAOI, it risks serotonin syndrome and a hypertensive crisis. It also overlaps poorly with SSRIs, SNRIs, stimulants, and bupropion [P5]. If you’re on an antidepressant, this single conversation is the difference between something managed and something dangerous.
Third, your psychiatric history, asked about not as box-ticking but because the trials that generated tesofensine’s safety data screened out people with that history, which means the public record genuinely has little to say about how the drug behaves in someone who carries it [P1]. A clinician who asks isn’t being nosy. They’re being honest about the limits of what’s known.
A process that says yes to everyone isn’t a referee. It’s a rubber stamp.
The dose as a decision, not a ceiling
Here’s where the “argues with itself” idea earns its keep a second time. Because the biggest number, that 10.6%, belongs to the dose that got dropped, a clinician acting in your interest isn’t chasing it. The doses that actually moved forward in development were the lower 0.25 mg and 0.5 mg, chosen specifically because they kept the cardiovascular cost within a range the developers found tolerable.
What that means, practically, is that good supervision often looks like starting lower and watching, rather than reaching straight for the number that reads best on a chart. Someone dosing a research-chemical powder alone has no such restraint built in, and no one whispering that the flashiest trial figure is exactly the one the company itself backed away from.
Where the referee actually matters: three months in
Every intake, no matter how careful, is a snapshot. Tesofensine’s real risk is a trend, and trends only show up if somebody keeps looking. This is where I think the word “supervised” earns its keep rather than just wearing it.
Real follow-up means someone checks how your heart rate and blood pressure have moved since you started, asks about the common complaints that turn up in the trial data (dry mouth, insomnia, nausea, headache, constipation, diarrhea), and adjusts the plan if something has drifted. If your resting pulse has crept upward or your blood pressure has climbed, follow-up is the moment somebody notices and does something about it, whether that’s lowering the dose or stopping altogether. None of that happens with a supplier whose relationship with you ended the moment your card was charged.
You can make this collaboration better, incidentally, by keeping your own simple record between visits: your dose, your resting heart rate, whatever symptoms show up. Walking into a check-in with actual numbers, rather than a general impression that you “think” you felt fine, turns the appointment from a guess into a genuine review. The tool doesn’t matter much. What matters is that this is a compound where the last several weeks of your body’s behavior are actually informative, and somebody, ideally both of you, needs to be paying attention to them.
An honest word about the friction
I don’t want to pretend any of this is frictionless, because that would be its own kind of dishonesty. The supervised route is slower than clicking “buy.” It involves an evaluation, a prescription, and check-ins, and even at the end of it you’re getting a compounded medication, not an FDA-approved finished drug. If you want tesofensine in hand tomorrow with nobody asking questions, this path will frustrate you.
But every piece of friction here is doing a specific job, the way a car’s speed limiter is doing a job even when you resent it on the highway. The intake catches the drug interaction. The conservative dosing keeps you off the ledge the developers themselves stepped back from. The follow-up catches the drift in your numbers before it becomes something worse. On a compound whose own creators couldn’t fully solve its heart-rate problem, that friction isn’t bureaucracy for its own sake. It’s the correction the drug needed, applied by a person instead of a pill.
It’s also worth being plain about where tesofensine sits, regulatorily, while you weigh all this. It is not FDA-approved. In the United States it’s classified as an investigational new drug. Its furthest step toward formal approval anywhere is a favorable opinion from a Mexican COFEPRIS technical committee in early 2023, which is not the same thing as an approval. There is no regulator’s sign-off doing the safety work for you here. That’s one more reason the human judgment in the loop isn’t optional.
What that supervision looks like when it’s done properly
So, concretely: what does a provider doing all of this correctly actually look like? It looks like a licensed telehealth clinic rather than a chemical seller. FormBlends is the clearest example of this model I can point to. Access runs through a clinician evaluation, a prescription written when it’s genuinely warranted, and dispensing through a licensed compounding pharmacy, with a monthly cost somewhere in the range of $90 to $300 depending on dose. Worth knowing, too: tesofensine is a small molecule, not a peptide, so it wasn’t caught up in the FDA’s recent peptide-compounding restrictions and remains available through licensed 503A pharmacies with a prescription. Everything walked through above, the baseline check, the medication review, the deliberate dosing, the follow-up, is what that structure exists to deliver. For anyone who wants to bring real data to a check-in, logging dose and symptoms between visits, using something like the FormBlends tracker app, meaningfully sharpens the follow-up. The app logs. It doesn’t prescribe and it doesn’t sell.
HealthRX (healthrx.com) runs on that same logic and belongs in the same supervised category: licensed clinical oversight first, medication dispensed through proper pharmacy channels rather than sold as a research chemical. Between the two, the practical question is which is licensed where you live, and whose intake and follow-up rhythm suits you.
And then there’s the contrast that makes the whole argument concrete: the research-chemical route, where tesofensine shows up as a “research use only” powder with no clinician attached, no prescription, and no one checking in afterward. None of what I’ve described happens there. Nobody takes your baseline. Nobody checks the vial against your antidepressant. Nobody is watching your heart rate three months from now, and nobody is reachable if something starts to move. The product carries no FDA verification of identity, strength, quality, or purity, so even the dose you think you’re managing is itself uncertain. That isn’t a discount version of supervised access. It’s simply the absence of the thing this particular drug requires.
Questions people actually ask
What will a clinician actually check before prescribing tesofensine? At minimum, your cardiovascular baseline, since the drug directly raises heart rate and blood pressure, and your full medication list, since it interacts dangerously with MAOIs, SSRIs, SNRIs, stimulants, and bupropion [P1][P5]. Psychiatric history matters too, because the original trials excluded people with one, leaving the mood-related effects under-studied [P1].
How often does follow-up actually need to happen? Often enough to catch a shift in heart rate or blood pressure and address side effects as they come up, which a clinician judges based on how you’re responding. The underlying point is that tesofensine’s chief risk is a number that can move over time, so checking back in is the whole point, not a formality after a single approval.
Why does the dose matter this much? Because the headline weight-loss figure, around 10%, came from the 1.0 mg dose that was dropped from development for cardiovascular reasons, while the doses that continued forward were the lower 0.25 mg and 0.5 mg [P1]. Careful dosing means matching the amount to what your body can tolerate, not reaching for the number that looks best in a trial summary.
Is tesofensine FDA-approved, so a doctor can just write for it like anything else? No. It’s classified in the US as an investigational new drug, not an approved one. Where it’s available, it comes as a compounded medication requiring a prescription, which is a large part of why clinical judgment and ongoing follow-up matter as much as they do.
What is tesofensine and how does it work?
Tesofensine is a triple monoamine reuptake inhibitor, meaning it blocks the reabsorption of dopamine, serotonin, and norepinephrine at once. That combination reduces appetite and, in some people, seems to modestly raise resting energy expenditure. It was originally studied for Parkinson’s and Alzheimer’s disease before researchers noticed substantial weight loss showing up as a side effect in trial participants. It has not cleared FDA approval for obesity as of this writing.
Does tesofensine actually burn fat, or does it just suppress appetite?
Both mechanisms seem to be at work, though appetite suppression is the better-documented one in the trial data. The norepinephrine piece may raise metabolic rate modestly, which could account for some fat loss beyond calorie reduction alone. Calling it a pure “fat burner” oversells what the current evidence supports. Most of the weight loss seen in trials is almost certainly a matter of people simply eating less.
Is tesofensine a peptide like semaglutide or tirzepatide?
No. Tesofensine is a small-molecule synthetic compound, not a peptide. Peptide drugs like semaglutide mimic gut hormones and act on GLP-1 receptors. Tesofensine works entirely through the central nervous system, by shifting neurotransmitter levels. The distinction matters clinically, because the side-effect profiles, cardiovascular considerations, and monitoring needs differ quite a bit between the two drug classes.
Where can someone actually get tesofensine legally?
Outside an active clinical trial, legal access in the United States is limited to compounded formulations prescribed by a licensed physician. Some physician-supervised compounding pharmacies, FormBlends among them, operate under state pharmacy board oversight and require a valid prescription along with ongoing monitoring before they’ll dispense anything. Anything sold as a research chemical or supplement online sits in a legally and medically gray zone, with no guaranteed purity, dosing accuracy, or safety follow-up built in.
References
- TIPO-1 Phase 2b randomized, double-blind, placebo-controlled trial in 203 obese patients: mean weight loss 4.5% / 9.2% / 10.6% at 0.25 / 0.5 / 1.0 mg vs 2.0% placebo over 24 weeks; heart rate +7.4 bpm at 0.5 mg; authors concluded the 0.5 mg result needs Phase 3 confirmation. Astrup et al., The Lancet, 2008. PMID 18950853. https://pubmed.ncbi.nlm.nih.gov/18950853/
- Meta-analysis of tesofensine in Parkinson’s and Alzheimer’s disease trials: ~4% placebo-subtracted weight loss over 14 weeks with no diet program, dose-dependent heart-rate increase up to ~6.8 bpm independent of weight loss. Astrup et al., Obesity (Silver Spring), 2008. PMID 18356831. https://pubmed.ncbi.nlm.nih.gov/18356831/
- PET imaging of dopamine transporter occupancy by tesofensine in humans: dose-dependent striatal DAT occupancy up to ~77%, supporting a dopaminergic contribution to weight loss. Appel et al., European Neuropsychopharmacology, 2014. PMID 24239329.
- Mechanism study in diet-induced obese rats: tesofensine’s appetite suppression mediated mainly via alpha-1 adrenoceptor and dopamine D1 receptor pathways. Axel, Mikkelsen, Hansen, Neuropsychopharmacology, 2010. PMID 20200509.
- Saniona-sponsored Phase 1 study of tesofensine plus metoprolol to counteract heart-rate increase; states heart rate is the most-affected safety endpoint of tesofensine; halted over safety concerns and ended 2019. NCT03488719.
- Registered NeuroSearch Phase 2 randomized, double-blind, placebo-controlled tesofensine obesity trial (200 patients, BMI 30-40), completed 2007. NCT00394667.